Aravind Eye Care System, Seva's partner in India, is the single largest eye care provider in the world, but they didn't get there just by helping themselves. This multi-part series examines Aravind’s external capacity building activities and the impact they have had on the organization itself. Over the next few months, stay tuned as we share this incredible story with you, piece by piece.
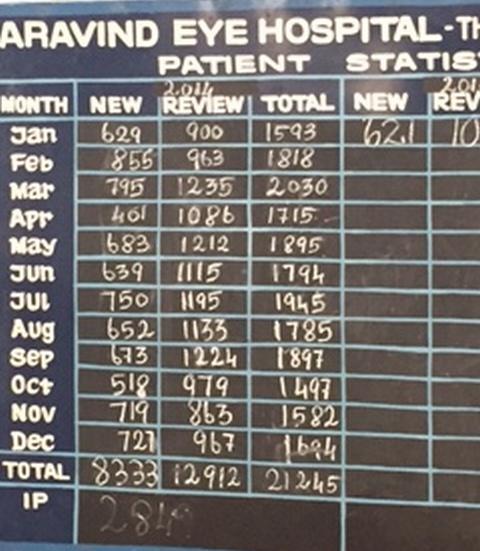
The Aravind Eye Care System (AECS) in Southern India has grown into a 4,000-bed, 10 hospital system that performs more than 350,000 eye operations and laser procedures annually, the largest single eye care provider in the world. Its growth and business model have received and continues to receive considerable attention from prestigious international business schools.
Along with its phenomenal internal growth, Aravind has also managed to help hundreds of other hospitals in many countries to increase their productivity and efficiency, far more than any other eye institution and arguably more than any other health institution in history. Almost undocumented, Aravind started providing this assistance to other hospitals, mostly free of charge, around 1992–93. It included absorbing the salaries and loss of service income since their own staff often had to travel offsite and be away for weeks or months at a time.

Helping others to improve productivity and efficiency, termed hereinafter ‘external capacity building’ may at first seem contrary to an institution’s competitive advantage of expanding its internal service capability. However, was Aravind’s external capacity building simply altruism or was it an essential, albeit unintended, factor driving its phenomenal internal success? We contend that Aravind’s external capacity building activities have had a significant impact not only with receiving institutions, but also on Aravind itself.
The Research
© Scott Burg
Seva Foundation and Seva Canada commissioned a case study of Aravind’s external capacity building program. Dr. Ken Bassett, Program Director for Seva Canada and independent researcher Scott Burg agreed to conduct the study. Mr. Burg traveled to Aravind to conduct formal interviews with Aravind staff, physicians and partners about the history, functions and motivation behind Aravind’s external capacity building operations.
Relevance to the World
This case study asks what benefit accrues to Aravind from systematically and extensively helping others? It identifies the range of capacity building activities, involving a cross section of hospital staff, assisting with everything from strategic planning to patient care and flow to floor cleaning and sterilization. We believe this study can provide lessons and inform practice and policy for clinics and hospitals worldwide. Readers within healthcare and other fields will no doubt be drawn to the many dimensions of this case and will want to learn how they too, can help themselves by helping others.

© Scott Burg
Hospitals around the world must drastically expand in order to provide services to ever increasing rural and urban populations. In order to meet demand, it is critical that these institutions operate productively and efficiently. At issue, is whether systematically helping institutions to help others can play a key role in their own, often much needed, development.
An Eye Care Problem
Nowhere is the need for increased efficiency and productivity more acute and its absence more tragic than in global eye care health. According to the latest reports of the World Health Organization (WHO), the total number of people with visual impairment worldwide was estimated at 285 million, of whom 39 million were blind, with 80% preventable, treatable or curable. Half of this blindness is due to cataract that can be cured with a 5–10 minute surgical procedure.
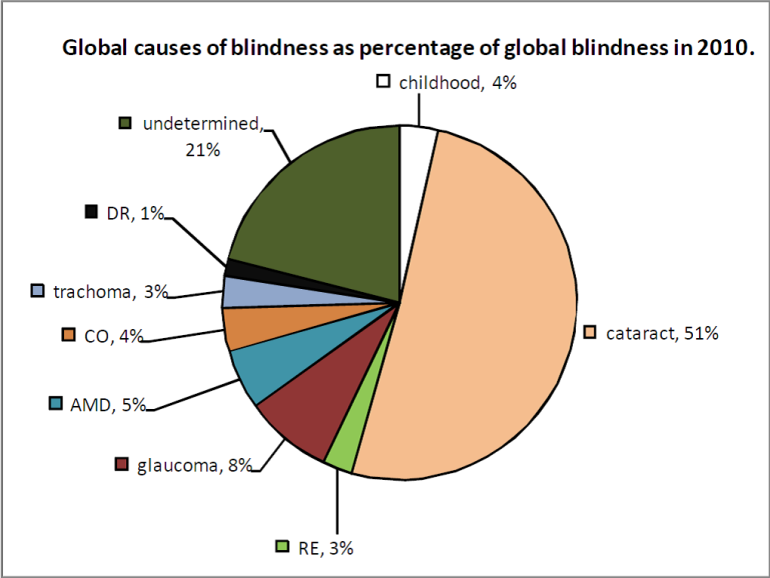
Ref: Pascolini D, Mariotti SPM. Global estimates of visual impairment: 2010. British Journal Ophthalmology Online First published December 1, 2011, as 10.1136/bjophthalmol-2011–300539. Figure 2B
Many institutions providing eye care in resource-poor areas around the world are significantly under-performing, with ophthalmologists often conducting fewer than 200 cataract operations per year. An ophthalmologist along with a well-managed team could perform as many as 2,000 cataract operations per year.
Over the next few months, we will be sharing this incredible story with you, piece by piece. Our primary goal is to disseminate this case study as broadly as possible, to encourage readers like yourself to share this story with others and to have organizations and individuals participate in the dialogue by contributing their own knowledge and experiences. We hope you will join us on this journey and help us share out the lessons and experiences reported here.
Future articles will include:
- History of development of AECS capacity building initiatives (internal and external).
- AECS internal training engagements, methodology and structure.
- Types of external capacity engagements within India and elsewhere.
- Lessons learned from capacity engagements.
- Challenges to conducting external capacity building.
- Future plans for capacity building.


